Your doctor checks your blood pressure, cholesterol, and blood sugar at every visit. But the single strongest predictor of how long you will live isn’t on that list — and most clinics don’t measure it at all.
There is a measurement that exercise physiologists have known about for decades, that major medical bodies have been quietly pushing into mainstream medicine, and that a growing body of research now regards as the single most powerful predictor of how long you will live. It is not your cholesterol. It is not your resting heart rate. It is not your BMI. It is your VO2max — the maximum rate at which your body can consume oxygen during intense exercise — and the data behind it are, by any reasonable standard, extraordinary.
In 2016, the American Heart Association published a landmark scientific statement making a formal argument that cardiorespiratory fitness — measured by VO2max — should be treated as a clinical vital sign, routinely assessed alongside blood pressure, cholesterol, and blood glucose. The statement drew on decades of large-scale epidemiological data and made a striking claim: low cardiorespiratory fitness is not merely associated with poor health outcomes — it is a more powerful predictor of mortality risk than smoking, hypertension, high cholesterol, or type 2 diabetes.
Most people have never had their VO2max measured. Many have never heard of it. Yet the evidence stacking up behind this number is, by now, difficult to ignore.
Key figures from the research
- 53% — reduction in all-cause mortality risk between the least fit and most fit groups in large studies
- 13–17% — reduction in all-cause mortality for every single MET increase in fitness level
- 122,007 — participants in the landmark JAMA study tracking fitness and long-term mortality
What VO2max Actually Measures
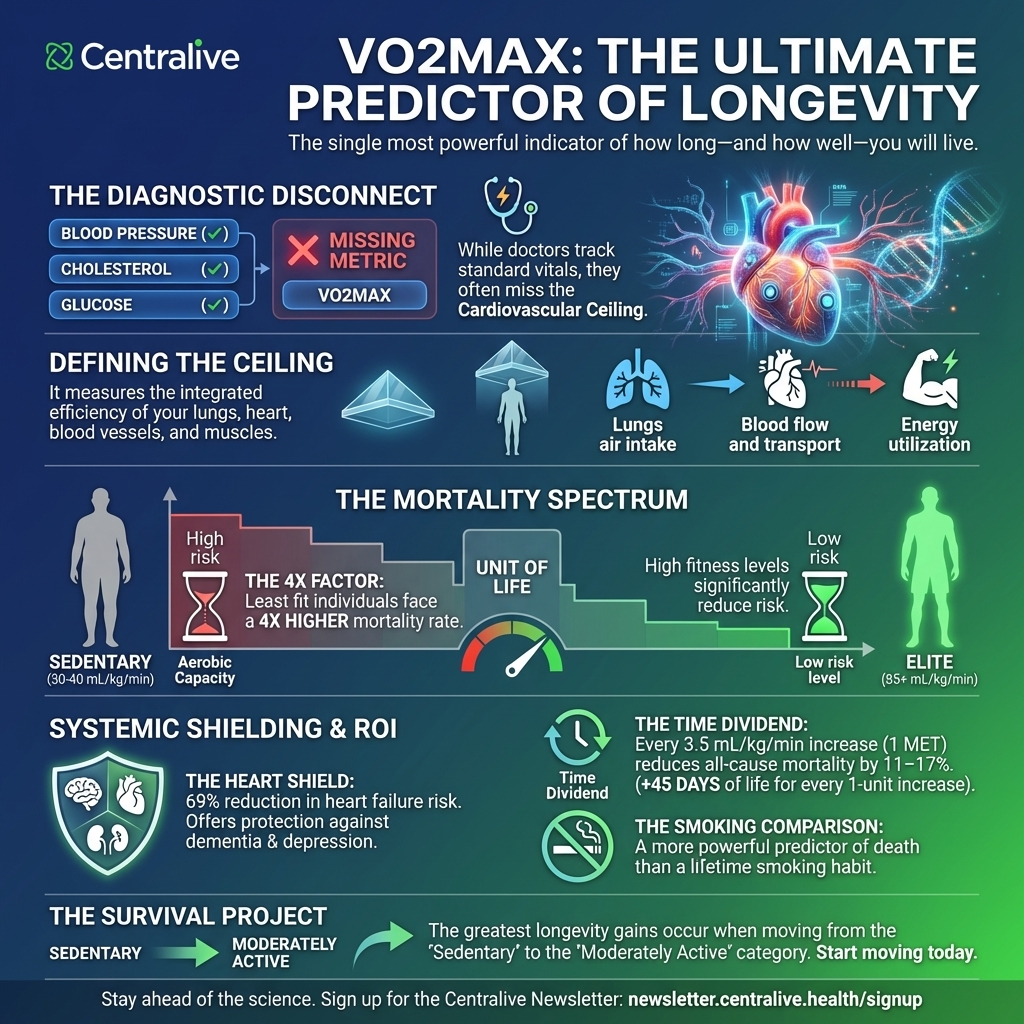
VO2max — maximal oxygen uptake — quantifies how much oxygen your body can extract, transport, and use during all-out exercise. It is expressed in millilitres of oxygen per kilogram of body weight per minute (mL/kg/min), and it captures, in a single number, the integrated performance of your lungs, heart, blood vessels, and muscles working together under maximum demand.
Think of it as your cardiovascular system’s ceiling. A higher VO2max means your heart can pump more blood per beat, your muscles can extract more oxygen from that blood, and your aerobic energy systems can sustain higher workloads for longer. In elite endurance athletes — Tour de France cyclists, cross-country skiers — values can exceed 85–90 mL/kg/min. The average sedentary adult in their forties sits somewhere between 30 and 40. The difference between those numbers is, in a very real sense, the difference between biological resilience and biological vulnerability.
“CRF is a potentially stronger predictor of mortality than established risk factors such as smoking, hypertension, high cholesterol, and type 2 diabetes mellitus.” — American Heart Association Scientific Statement, 2016
The Mortality Data Is Hard to Dismiss
The evidence linking VO2max to longevity has been building since the 1980s, when Steven Blair and colleagues at the Cooper Institute tracked more than 13,000 people over time and found that those in the bottom fifth of cardiorespiratory fitness had two to three times the mortality risk of those in the top fifth — a relationship that held even after adjusting for smoking, blood pressure, and cholesterol.
In 2018, a study published in JAMA Network Open brought this question into sharper focus. Researchers measured VO2max in 122,007 adults undergoing exercise treadmill testing, then followed them for years. The results were striking: people in the lowest fitness category had a mortality rate nearly four times higher than those in the highest. The difference between low and below-average fitness alone was larger than the mortality risk attributed to smoking, diagnosed heart disease, or hypertension in the same dataset.
How VO2max compares to traditional risk factors (relative mortality risk increase):
- Low fitness vs. high fitness — approximately 4× higher mortality risk
- Below-average fitness — approximately 2.7× higher
- Smoking — approximately 1.4× higher
- Diagnosed heart disease — approximately 1.3× higher
A 2024 overview of meta-analyses published in the British Journal of Sports Medicine, drawing on data from over 20.9 million observations across 199 cohort studies, confirmed the relationship is robust, consistent across populations, and dose-dependent — every incremental improvement in fitness reduces risk.
Key finding: Every 1-MET increase in cardiorespiratory fitness (equivalent to approximately 3.5 mL/kg/min of VO2max) is associated with an 11–17% reduction in all-cause mortality risk. This is not a threshold effect — the benefit is continuous, and it extends across the full range of fitness levels.
Perhaps most striking of all is what the data show about the shape of the risk curve. The American Heart Association’s analysis found that more than half of the entire reduction in all-cause mortality occurs between the least-fit group and the next least-fit group. The biggest gains are not reserved for elite athletes. They belong to the people who move from sedentary to simply active.
Why VO2max Predicts More Than Heart Disease
One of the more counterintuitive findings in this literature is how broadly VO2max predicts health outcomes — far beyond cardiovascular disease. The 2024 British Journal of Sports Medicine overview found that high cardiorespiratory fitness was associated with large risk reductions not just for heart attack and stroke, but for heart failure (69% reduction in risk), kidney disease, depression, dementia, and Alzheimer’s disease. The relationship extends to cancer outcomes as well: low fitness is associated with increased risk of several cancers, and higher fitness improves survival odds after diagnosis.
The biological mechanisms are not fully resolved, but the working explanation involves several converging pathways. Higher VO2max reflects a more efficient cardiovascular system — lower resting heart rate, better cardiac output, improved vascular elasticity — which reduces the chronic strain associated with cardiovascular disease. It is also associated with better metabolic regulation (glucose sensitivity, insulin response, lipid profiles), lower systemic inflammation, and, more recently, longer telomeres — the protective caps on chromosomes that shorten with biological aging. A 2025 systematic review and meta-analysis found that people with higher VO2max had significantly longer telomeres than those with low fitness, suggesting that aerobic capacity may operate as a brake on cellular aging itself.
The Vital Sign Nobody Measures
Here is the paradox at the heart of this story. The evidence that VO2max predicts longevity better than blood pressure, cholesterol, or smoking status has been accumulating for more than thirty years. The American Heart Association formally called for it to be assessed as a clinical vital sign in 2016, with a follow-up paper in 2024 reiterating that conclusion with even stronger evidence. And yet most people reading this article will never have had their VO2max measured by a doctor.
Why VO2max remains out of routine clinical practice:
1. Testing requires specialist equipment. A gold-standard VO2max test requires a metabolic analyser, a treadmill or cycle ergometer, and trained staff — making it expensive and logistically demanding for most primary care settings.
2. It isn’t in the risk calculators. Cardiorespiratory fitness is not included in standard cardiovascular risk calculators, meaning clinicians have no formal protocol for integrating it into routine risk stratification.
3. The only remedy is exercise. Unlike cholesterol or blood pressure, there is no pharmacological intervention for low VO2max — the only remedy is exercise, which sits outside the traditional prescribing model.
4. Clinical adoption lags technology. Submaximal tests, non-exercise algorithms, and consumer wearable estimates can now approximate VO2max in everyday settings — but clinical validation and adoption have not kept pace.
This last point opens a door. A growing body of research is investigating whether VO2max estimates derived from consumer wearables — the same devices that sit on tens of millions of wrists — are accurate enough to be clinically useful. The picture is mixed, but the direction of travel is clear: the barrier to regular VO2max monitoring is coming down, and with it, the potential to bring one of medicine’s most powerful prognostic tools to a mass audience for the first time.
What This Means for You
The literature on VO2max and mortality carries an unusually practical message, which is that fitness is not an aesthetic project. It is a survival project. The difference in all-cause mortality between the least fit and the most fit groups in large studies is larger than the mortality impact of smoking. It exceeds the risk from diagnosed cardiovascular disease. And crucially, the benefit is not front-loaded at the elite end — it accumulates most steeply among people making the transition from inactive to moderately active.
Every unit of improvement in VO2max — achievable through consistent aerobic exercise, even at modest intensities — translates directly into reduced mortality risk. Not modestly reduced. Not marginally reduced. Reduced by 13 to 17% per additional MET of fitness capacity, in study after study, across millions of participants, over follow-up periods stretching to 46 years.
The Copenhagen Male Study, which tracked participants over 46 years using Danish national death registers, found that each unit increase in VO2max was associated with 45 additional days of life. That is not a metaphor. It is a number derived from one of the longest and most carefully controlled fitness studies ever conducted.
For medicine, the implication is that a routine, affordable estimate of cardiorespiratory fitness belongs in clinical practice — not as an optional add-on, but as a standard part of the risk conversation that happens between doctor and patient. For the rest of us, the implication is simpler: the number on your wrist or in your lab results that most closely approximates your VO2max may well be the most important health metric you are currently ignoring.
Sources: Ross et al., American Heart Association / Circulation (2016 & 2024); Mandsager et al., JAMA Network Open (2018); Lang et al., British Journal of Sports Medicine (2024); Ryall & Denham, The Journals of Gerontology (2025); Loe et al., Journal of the American College of Cardiology (2018).