Almost every consumer sleep wearable was built and validated around a single assumption: a healthy adult sleeping one consolidated bout at night, alone, on a regular schedule. That assumption holds for a lot of people a lot of the time, which is why devices look so accurate in validation papers. The trouble starts when your study population does not match it. Night-shift nurses sleeping at noon, students taking afternoon naps, couples sharing a bed, and anyone with a chaotic schedule all violate the design assumptions in ways that quietly distort the data. This post walks through the four situations researchers ask about most, explains why each one breaks the algorithm, and lays out how to design around it.
The one assumption that breaks everything
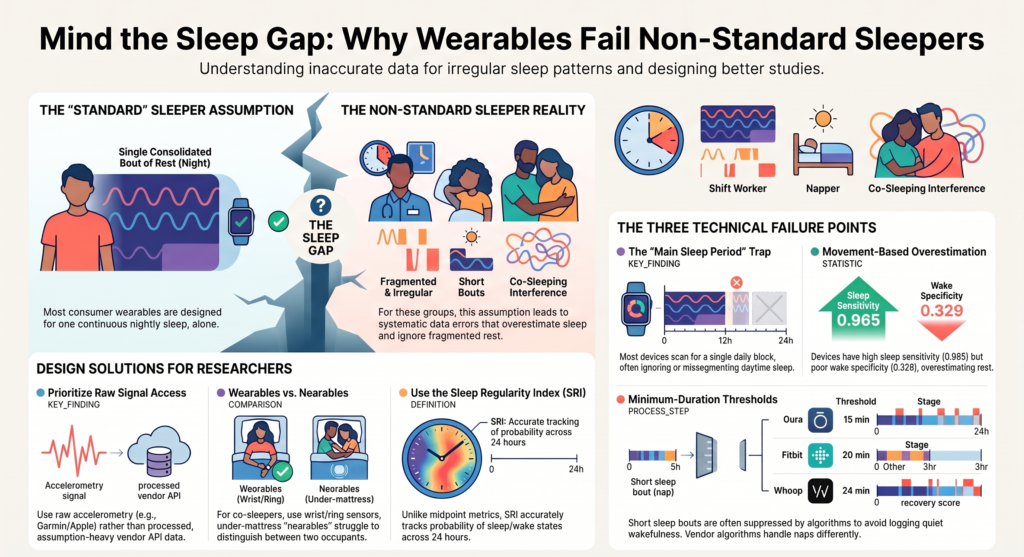
Three mechanisms inside a typical sleep wearable fail in non-standard sleep, and they tend to fail together. The first is the auto-detected “main sleep period.” Most devices scan the day, pick the single block they believe is your real sleep, and report on that. The 2024 Sleep Research Society state-of-the-science review is blunt about how approximate this is, noting that automatically determined sleep times are an estimate based on the first and last sleep-to-wake transitions and should be used with caution, and that some devices output multiple sleep periods following proprietary logic that may segment incorrectly.1
The second mechanism is the minimum-duration threshold. Devices suppress short sleep blocks to avoid logging every time you sit still, which means naps below a cutoff simply never appear. The third is the oldest problem in the field: movement-based wake detection. The basic assumption of actigraphy is that motion means wake and stillness means sleep, which produces a well-documented imbalance. In the canonical wrist-actigraphy validation by Marino and colleagues, across more than 232,000 epochs, sensitivity for detecting sleep was 0.965 but specificity for detecting wake was only 0.329.2 In plain terms, these devices are excellent at spotting sleep and poor at spotting quiet wakefulness, so they systematically overestimate sleep. That error grows as sleep becomes more fragmented, which is exactly what happens in the situations below.
Shift work and daytime sleep
Daytime sleep is the clearest example of the main-sleep-period assumption causing trouble. The underlying movement signal is still there during the day, so a raw-data algorithm can score it, but accuracy degrades. A polysomnography-validated study of simulated shift work found that daytime versus nighttime status affected specificity and overall agreement but not sensitivity, with specificity lower for daytime sleep across the algorithms tested, and all algorithms overestimating total sleep time.3
The bigger issue for consumer devices is that their accuracy in shift workers is largely unknown, because the validation work that exists captured nighttime sleep. The 2024 review states directly that while consumer wearables have been assessed in shift workers, the captured sleep was during the night, so the ability of these devices to estimate daytime sleep in shift workers or people with circadian rhythm disorders remains unknown.1 Even the most substantial consumer validation in this population, a study of first-responder police and paramedics, recorded its polysomnography comparison at night, and its authors recommended that the device would be more useful for research with open-source algorithms and raw data access.4
On the analysis side, open-source pipelines handle 24-hour data more gracefully than vendor apps, but only if you configure them to. The widely used GGIR package detects a daily sleep-period time window from raw accelerometry without a diary,5 but by default it looks for the main daily sleep period and does not detect sleep outside that window. For genuine daytime sleepers, you need to inspect 24-hour actograms and anchor the analysis with a diary or event marker rather than trusting automatic detection.
Naps and short sleep bouts
Naps fall into the gap created by minimum-duration thresholds, and those thresholds vary enough between devices to change your results depending on which one you pick. Published and vendor-documented behavior includes the following:
- Fitbit needs at least 3 hours of sleep to estimate sleep stages, so shorter naps get no staging, and it records naps of at least 20 minutes as a basic “Other sleep” category. It treats daytime sleep the same as nighttime sleep once detected.
- Oura auto-detects naps longer than 15 minutes and under 3 hours, reclassifies anything over 3 hours as a main sleep period, and provides a full stage breakdown for naps.
- WHOOP auto-detects sleep longer than 1 hour, logs shorter periods as naps from around 24 minutes, and generates stages for naps but no recovery score.
- Apple Watch added automatic nap detection in watchOS 11 in 2024, but the nap feature does not classify sleep stages.
- GGIR uses a default minimum sleep-period length of 60 minutes, so shorter naps are excluded unless you change the setting.
Direct nap-detection accuracy is poor where it has been measured. The 2024 review summarizes a laboratory study in which a device correctly identified only 6 of 20 daytime naps while correctly detecting 24 of 30 nighttime sleep periods, and notes that missed daytime sleep episodes were most likely when the daytime time-in-bed period was short.1 If naps are an endpoint in your study, the device threshold is not a footnote, it is a primary methodological decision.
Sleeping with a partner or a pet
Here the sensor location matters more than the algorithm. Wrist-worn and ring devices sense the wearer’s own motion, so they are relatively robust to a partner shifting in bed. Non-contact options are the opposite case. A comprehensive review of home sleep monitoring technologies notes that shared beds introduce measurement errors and that smart mattresses may struggle to differentiate between two occupants.6 Under-mattress and radar-style “nearable” sensors are designed to read movement in the bed itself, which is precisely what makes a restless partner, a child, or a pet so disruptive to them.
The effect is measurable even for the wearer’s own non-standard sleep. An under-mattress sensor validated against polysomnography across more than 400 nights classified about 91 percent of sleep but only half of wake at night, and during daytime sleep its wake classification fell to roughly a quarter while sleep classification stayed high.7 For bed-sharing or co-sleeping cohorts, the practical takeaway is to prefer wrist or ring wearables and, if a nearable is unavoidable, to record co-sleeping as a covariate.
Irregular and fragmented schedules
Standard sleep metrics assume one main sleep period per day, so they degrade badly under highly variable timing, polyphasic sleep, or social jetlag. The right tool here is the Sleep Regularity Index, which measures the probability that a person is in the same state, asleep or awake, at any two time points 24 hours apart, scaled from 0 for random to 100 for perfectly regular.8 Its key advantage is that, unlike conventional regularity measures built on a single sleep midpoint, it does not rely on one main sleep period, which makes it suitable for people with multiple sleep episodes across the day, including shift workers and habitual nappers.
Two practical points when you use it. First, give it enough data: regularity metrics tend to overestimate regularity when based on a week or less, and at least 5 valid days is a common minimum criterion.9 Second, remember the specificity problem from earlier. Fragmented nights are exactly where movement-based devices over-score sleep, so total sleep time and sleep efficiency should be interpreted as likely overestimates in this group.
The decision that sits underneath all four
Every one of these situations comes back to the same lever: are you analyzing a vendor’s proprietary processed output, or the raw signal? Processed outputs bake in the nighttime, consolidated, single-sleeper assumptions and auto-detect one main sleep period, so for a napper or a shift worker they may simply return nothing for the sleep you care about. Raw accelerometry and raw photoplethysmography let you run your own 24-hour, assumption-free sleep detection and define the sleep periods yourself.
This maps directly onto the access model of the platform you choose, and it is the distinction we build on at Centralive. We provide raw signal access through the SDKs of platforms such as Garmin and Apple, rather than relying on the processed outputs of API-only platforms like Oura, which return aggregated sleep periods rather than the underlying signal. Garmin in particular is a strong first-class research platform here: its Health Companion SDK exposes raw accelerometer and beat-to-beat data, without a subscription model and across accessible hardware. With the raw signals in hand, a research team can run a single open-source, version-controlled pipeline, such as GGIR with the van Hees sleep-period algorithms, configured for the population at hand rather than for an idealized nocturnal sleeper.
Practical recommendations
- Decide raw versus processed at the design stage. If your cohort includes shift workers, nappers, or irregular sleepers, prioritize raw-signal access and do not rely on vendor main-sleep auto-detection as your primary endpoint.
- Anchor sleep periods with a diary, an event-marker button, or ecological momentary assessment, since auto-detected windows are unreliable in non-standard sleep.
- For bed-sharing or pet co-sleeping cohorts, prefer wrist or ring devices over under-mattress or radar sensors, and log co-sleeping as a covariate if a nearable is unavoidable.
- For nap studies, confirm and where possible adjust each device’s minimum-duration threshold, and expect short naps to be missed or left unstaged.
- For irregular or shift-work cohorts, report the Sleep Regularity Index alongside duration and efficiency, require at least 5 valid days, and treat total sleep time as a likely overestimate.
- Performance-evaluate the specific device, firmware, and population against polysomnography or research actigraphy before trusting endpoints, using multi-night designs. Healthy-adult nighttime accuracy does not transfer automatically to these groups.
The honest summary is that wearables do not handle unusual sleep well out of the box, because out of the box they assume the sleep is not unusual. But the failure is predictable, which means it is designable around. Get to the raw signal, choose the sensor location that suits the sleeping arrangement, pick metrics that do not assume one sleep period a day, and validate in the population you actually have rather than the one the device was built for.
References
- de Zambotti M, Goldstein C, Cook J, Menghini L, Altini M, Cheng P, Robillard R. State of the science and recommendations for using wearable technology in sleep and circadian research. Sleep. 2024;47(4):zsad325. doi:10.1093/sleep/zsad325. https://doi.org/10.1093/sleep/zsad325
- Marino M, Li Y, Rueschman MN, et al. Measuring sleep: accuracy, sensitivity, and specificity of wrist actigraphy compared to polysomnography. Sleep. 2013;36(11):1747-1755. doi:10.5665/sleep.3142. https://doi.org/10.5665/sleep.3142
- Quante M, Mariani S, Weng J, et al. Actigraphy-based sleep detection: validation with polysomnography and comparison of performance for nighttime and daytime sleep during simulated shift work. Nature and Science of Sleep. 2022;14. doi:10.2147/NSS.S373107. https://doi.org/10.2147/NSS.S373107
- Stone JE, Sletten TL, Magee M, et al. Validation of the Fitbit Charge 2 sleep and heart rate estimates against polysomnographic measures in shift workers: naturalistic study. Journal of Medical Internet Research. 2021;23(10):e26476. doi:10.2196/26476. https://doi.org/10.2196/26476
- van Hees VT, Sabia S, Jones SE, et al. Estimating sleep parameters using an accelerometer without sleep diary. Scientific Reports. 2018;8:12975. doi:10.1038/s41598-018-31266-z. https://doi.org/10.1038/s41598-018-31266-z
- Pan Q, et al. A comprehensive review of home sleep monitoring technologies: smartphone apps, smartwatches, and smart mattresses. Sensors. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11945902/
- Manners J, Baker A, Lovato N, et al. Performance evaluation of an under-mattress sleep sensor versus polysomnography in over 400 nights with healthy and unhealthy sleep. Journal of Sleep Research. 2025;34(6):e14480. doi:10.1111/jsr.14480. https://doi.org/10.1111/jsr.14480
- Phillips AJK, Clerx WM, O’Brien CS, et al. Irregular sleep/wake patterns are associated with poorer academic performance and delayed circadian and sleep/wake timing. Scientific Reports. 2017;7:3216. doi:10.1038/s41598-017-03171-4. https://doi.org/10.1038/s41598-017-03171-4
- Fischer D, Klerman EB, Phillips AJK. Measuring sleep regularity: theoretical properties and practical usage of existing metrics. Sleep. 2021;44(10):zsab103. doi:10.1093/sleep/zsab103. https://doi.org/10.1093/sleep/zsab103
Sign up for the Centralive Newsletter: https://newsletter.centralive.health/signup